VTS Bone Graft Helps A Chihuahua Mend A Jaw Fracture at Sierra Veterinary Specialists
Sierra Veterinary Specialists
Periodontal Disease Case Study – Use of an alloplast material to treat a 309 furcation defect
Dr. David Clarke, BVSc, ADVC, fellow AVD, MANZCVS
Dental Care for Pets
Hallam, Victoria, Australia
Dental Implants and Incisor Bridge Placement in a Dog
From Journal of Veterinary Dentistry
REQUEST FULL ARTICLE
Rudy is a 10 year old Havanese patient of Dr. John Lewis (NorthStar Vets, Robbinsville, NJ). His tumor, an odontogenic fibrosarcoma, was treated by resection and replacement with allograft. View Dr. Lewis’ video detailing the case history here. As of this writing, the 7 week follow up shows that “things are going great” for Rudy!
Another study detailing successful use of VTS’ cortical allograft struts has been recently published by Drs. Chris Snyder, Jason Bleedorn and Jason Soukup (Successful Treatment of Mandibular Nonunion with Cortical Allograft, Cancellous Autograft, and Locking Titanium Miniplates in a Dog, Journal of Veterinary Dentistry, 33(3):160-169, 2016.) See Case Study
Guided Tissue Regeneration in Four Teeth Using a Liquid Polymer Membrane
from Journal of Veterinary Dentistry
Successful Treatment of Mandibular Nonunion With Cortical Allograft, Cancellous Autograft, and Locking Titanium Miniplates in a Dog
from Journal of Veterinary Dentistry
Bone Graft for Periodontal Disease in a Miniature Poodle Dog
Dr. Brett Beckman
Atlanta, GA
This case courtesy of Dr. Rocco Mele, DVM assisted by Emily Schmidt, CVT, BS of Eastpoint Pet Clinic in Tucson, Arizona, photography by Cathy Mele
Dental specialists and general practice veterinarians alike are familiar with the difficult task of treating periodontal disease in canines and felines – whether it be through extractions, guided tissue regeneration, or a basic oral hygiene regimen. When full-mouth or multiple extractions are a surgeon’s only option, Veterinary Transplant Services’ injectable bone putty, Fusion Xpress, can assist with bone and soft tissue regrowth and help your patients heal stronger!
Sophie, a 13-year-old terrier mix, presented to Dr. Rocco Mele with grade 4 periodontal disease that necessitated extraction of several teeth.

Bone loss surrounding the roots of Sophie’s molars can be seen on radiography taken at her initial consultation. Her mandibular bone height is decreased, leaving these teeth unstable and her mandible prone to fracture.
Dr. Mele’s recommendation for Sophie, to prevent pathologic fracture of her mandible and further bone loss in her surrounding teeth was the surgical extraction of the diseased molar and premolar (which was also suffering bone loss, with both interior and exterior resoprtion taking place).
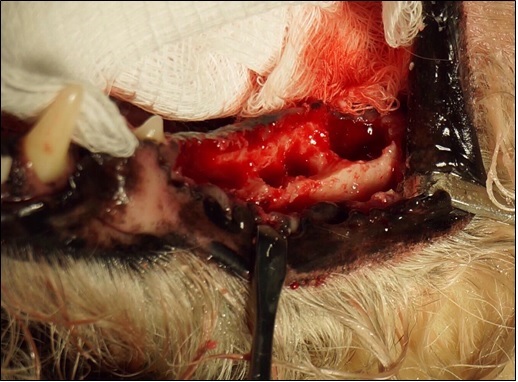
This photograph, taken intra-operatively following surgical extraction, shows the extent of the bone loss in Sophie’s mandible. Prior to the placement of Fusion Xpress, the site is fully debrided and irrigated to reduce potential for bacterial growth.
Fusion Xpress is the perfect solution for these hard-to-reach surgical sites. Made of a combination of equine bone and our synthetic bone substitute, Synergy, and packaged in individual doses in regular luer-tip syringes, Fusion Xpress can be expressed directly into a surgical site. Fusion Xpress‘ putty carrier makes it possible for the graft to stay in place while irrigating and regardless of the shape or size of the defect.

Fusion Xpress in place. This image, of another patient receiving periodontal surgery, illustrates the utility of the putty to mold to unique defects and stay in place even in bloody or irrigated sites.

Following graft placement, flaps can be opposed and the site surgically closed. Closure can happen immediately after graft placement – no drying or setting time is required.
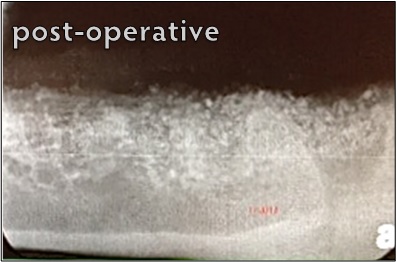
Both the particles of the equine bone and the synthetic are visible on the radiograph of the mandible immediately post-operative.
Sophie was seen for a recheck appointment 18 months following surgery.
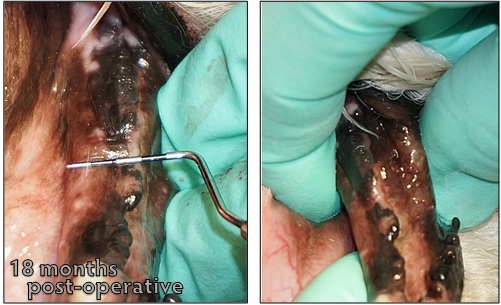
On physical exam, a probe held over the mandibular ridge shows a width of nearly 12mm. The robust bone growth is further illustrated when the surgeon grasps the mandible to isolate the mandibular ridge from the surrounding soft tissue.
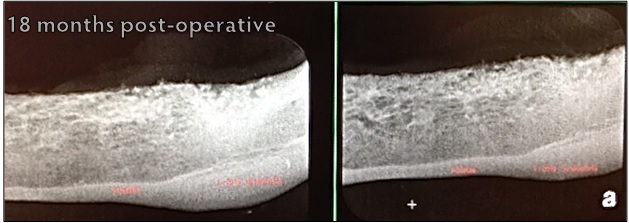
Two-view radiographs of the mandible reveal strong, radiopaque bone growth in the areas previously marred with bone loss secondary to Sophie’s periodontal disease. Both images were taken at the same visit.
Help your patients fight bone loss with Fusion Xpress – it’s easy to apply, offered in a variety of sizes and at a price that can fit any practice. Packaged in single-use doses, our putty is stored at room temperature and has a two-year shelf-life. Let VTS help you help your patients beat periodontal disease!
Case courtesy of Dr. Jan Bellows, DVM, AVDC, ABVP of All Pets Dental in Weston, FL.
Furcation defects are areas of bone loss, usually resulting from periodontal disease, in which the areas between a tooth’s roots are either exposed or inadequately protected. These defects are often treated through surgical extraction of the affected tooth. However, with the help of VTS’ graft products, surgical extractions aren’t the only option for veterinarians and pet owners.
Guided bone regeneration is a procedure that directs growth of bone to a site. In the case of a furcation defect, these procedures can help to strengthen the bone surrounding the defect. This was the case for a Golden Retriever who was referred to Dr. Jan Bellows. This pet’s owners wanted to do anything they could to save a tooth that another veterinarian wanted to extract. Dr. Bellows recommended she undergo a guided bone regeneration procedure. This patient had similar defects bilaterally. One side, unfortunately, had to be extracted. For the side pictured, Dr. Bellows used VTS’ Synergy and a cancellous mini block.
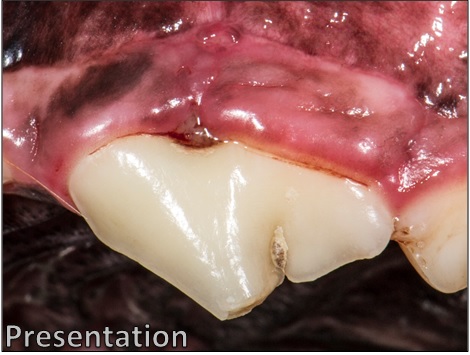
At the patient’s initial consult, the gingival tissue surrounding the tooth is visibly swollen and inflamed. Plaque and blood can be seen surrounding the defect. This tooth is also affected with an uncomplicated crown fracture.

At the time of referral, the defect had progressed to a stage 3 furcation defect.The soft tissue has recessed to the point that the defect is fully exposed; and a probe can be inserted in one side of the defect and come out the other.

Bone loss is apparent in this pre-operative radiograph. Note the difference between the area of the defect, and the same area on another tooth on the left-hand side of the film.
Following the surgical extraction of the other tooth, the guided tissue and bone regeneration process begins on the tooth to be saved.
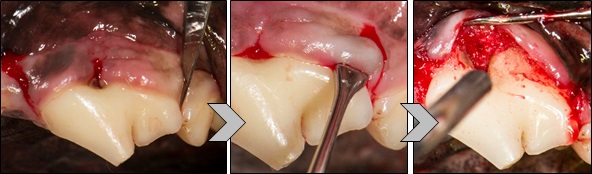
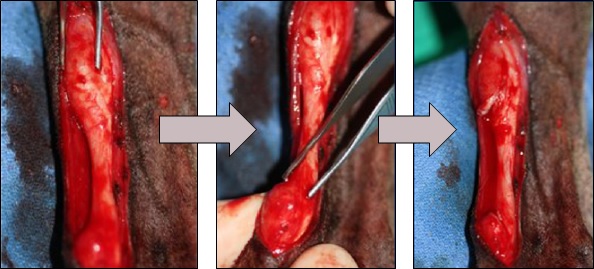
First, incisions are made on either side of the defect using a scalpel. The soft tissue is then separated from the tooth to fully expose the defect.

The defect is fully irrigated and cleaned to prepare for graft placement. With periodontal disease like this, it is common for food and bits of plaque to become lodged in the defect, causing further infection, irritation, and bone loss. Fully irrigating and debriding the defect removes the debris and prepares the root for regeneration of the periodontal ligament, which is expected with good root planing and bone grafting.
VTS’ cancellous mini blocks measure approximately 0.5 cm x 0.5 cm x 0.8 cm and are ideal for use in dentistry. Cancellous blocks are made from dense cancellous bone typically found in the condyles and plateaus of femur and tibia.
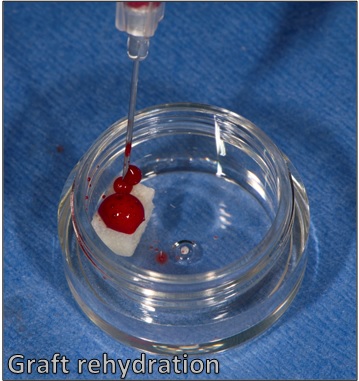
VTS’ cancellous mini blocks are shipped freeze-dried and must be rehydrated prior to use. Ideally, whole blood taken peripherally or from a bleeding surgical site can be used to rehydrate the graft. If the surgeon is unable to obtain whole blood, sterile saline may be used.
Once the graft has been rehydrated, it can be cut, shaved, or burred to the size and shape the surgeon prefers or works best for the patient. For this case, Dr. Bellows cut the block into a small slice that fit directly into the defect, and then smaller pieces to be packed on top.
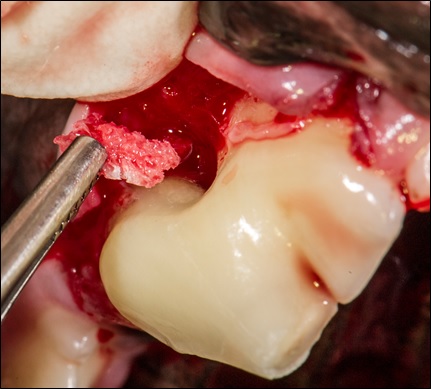
The cut and shaped mini block “slice” is placed into the defect site using surgical forceps.

The remaining block pieces packed over the defect.
Dr. Bellows then packed VTS’ synthetic bone graft, Synergy, rehydrated with blood, over the defect site, and into any void left by the soft tissue flap.

The flap is then closed over the surgical site.
Extraction isn’t always the only option for pets with furcation defects. Bone graft is the best substrate for remodeling and reformation of a patient’s lost bone stock. As advances in veterinary dentistry continue, VTS wants to help veterinarians save teeth!
In addition to providing the particulate allografts, injectable bone putty, and synthetic bone grafts you love – VTS also provides a variety of soft tissue grafts, including tendon allografts for orthopaedic use.
Stay tuned for more case studies involving soft tissue grafts.
Case courtesy of Dr. S. Gary Brown, DVM, DACVS of Veterinary Orthopedic and Surgery Service in Fremont, CA.
Devo, a 3.5 year-old Whippet, was referred to Dr. Brown for an injury to his right hind limb that was a result of being struck by his owner’s electric mobility scooter. Devo was placed on moderate exercise restriction immediately following the injury. A week later, Devo was still limping and there was a swelling over his right Achilles tendon. Devo was placed on an NSAID, given Acepromazine for sedation, and was placed on strict exercise restriction. When Devo’s limp was not improving with pharmaceuticals, it was time for an evaluation by an orthopaedic specialist.
On evaluation by Dr. Brown, Devo was found to have a severed Achilles and SDF tendon. Dr. Brown recommended repair using an allograft tendon from VTS.

In this pre-operative photograph, initially taken for measurement purposes, swelling is seen at both the proximal and distal ends of the Achilles tendon. The swellings are the ends of the severed tendons that have been unapposed and unable to heal in the weeks since Devo’s injury.
The first step of the surgery was to fully debride the collagen and connective tissue that had formed around the injury site. When fully debrided, the severed ends of the damaged tissues are suitable for graft implantation.
VTS’ tendon allografts are shipped frozen, on dry ice, and have a six-month shelf life. Prior to the procedure, the graft is removed from the freezer and allowed to thaw to room temperature for implantation. For this procedure, Dr. Brown used a superficial digital flexor tendon, our most common selection for Achilles (common calcaneal) tendon repairs.
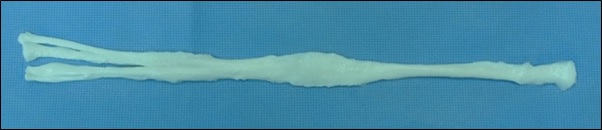
SDF allograft tendon.
Once the site is fully cleaned, flushed, and debrided, the allograft can be sutured to the ends of the severed tendon. For this particular procedure, Dr. Brown made an incision in the allograft at one end of the tendon so that there was a “Y” shape on both ends.

The proximal “Y” end of the tendon is sutured to the remnant of the injured tendon. The Y-shape allows for a stronger repair as there are more points of contact between the allograft and the existing tendon structure.
Once the proximal end of the tendon is in place, the distal end can be sutured. Dr. Brown pulled the allograft tight to ensure that it was the approximate length of the injured tendon, allowing 5 degrees of extra extension.

Once the allograft has been stretched tight and the proper angle has been achieved, the distal ends of the tendon are sutured to the remnants of the injured tendon tissue.

The tendon is then sutured to the remaining tendons in the surgical site. For this procedure, Dr. Brown used 3-0 nylon suture. While nylon is durable, as Devo healed, the knots began to protrude slightly from the skin and were eventually removed. Dr. Brown now recommends PDS with knots cut short and turned downward for these procedures.
Devo recovered very well from his surgical procedure. He spent six weeks in a padded splint that fully immobilized the tendon and hock joint. Some surgeons use an external fixator to ensure that the site remains immobilized as the tendon heals. However, Dr. Brown’s use of the splint serves a similar purpose that fit well with this active dog’s lifestyle.

Devo’s splint from the front and rear. The splint allows him to ambulate (slowly and controlled) while still protecting the surgery site.
Patients with tendinopathies and tendon injuries are often given a poor prognosis or are subjected to months and months of rehabilitation and therapy. However, with an allograft transplant, these patients can fully recover and return to their normal activity level. çevrimsiz bonus
Devo is now five years from his initial surgery and, per Dr. Brown, has fully recovered and has a fully-functioning hock.
Have patients who can’t seem to keep their tendons tight? It’s time for a transplant!